Not All Brain Swelling Is Equal in Venous Stroke
Key Takeaway: In patients with cerebral venous thrombosis—a rare but serious type of stroke—the specific pattern of brain edema identified on initial imaging dramatically shapes the prognosis. Cytotoxic edema, in particular, has been observed to increase the likelihood of in-hospital death by more than threefold, suggesting that not all “brain edema” carries the same weight when clinicians make early treatment decisions.
An Unconventional Stroke Presentation
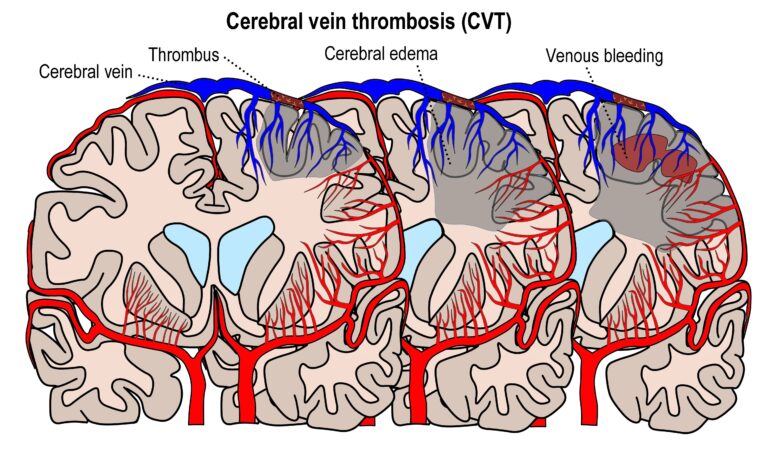
In patients facing a rare yet dangerous type of stroke, the specific pattern of edema on initial brain imaging can increase the risk of in-hospital mortality more than threefold. That sentence alone should give any emergency physician pause. Although cerebral venous thrombosis (CVT) accounts for less than 1% of all strokes, it disproportionately affects young adults, women using oral contraceptives, and patients with inherited clotting disorders[2]. Unlike a classic arterial stroke, caused by a blocked artery cutting off blood flow, CVT occurs when a blood clot forms in the venous drainage system—the large sinuses and veins responsible for carrying blood out of the skull. The result is a buildup of pressure, congestion, and, frequently, brain edema. But it is here that the story becomes more nuanced than many clinicians realize: the character of that edema is of paramount importance.
Study Methodology
A team of researchers analyzed a registry database containing data from 394 patients diagnosed with CVT. Rather than lumping all cases of brain swelling under a single heading like “cerebral edema,” the investigators meticulously categorized the edema on each patient’s initial brain imaging into distinct subtypes. The two subtypes that revealed the sharpest clinical distinctions were cytotoxic edema, which stems from true cellular injury and death, and vasogenic edema, which results from fluid leaking from a compromised blood-brain barrier without immediate cell destruction. The researchers also tracked whether the edema was localized or diffusely spread across the brain in a pattern called global cerebral edema. Outcomes were monitored at two critical time points: in-hospital mortality and six-month functional status, measured using standard disability scales.
Findings
More than half of the registry patients were found to have developed some form of cerebral edema—a striking prevalence that highlights just how common this complication is in CVT. The outcomes, however, diverged sharply depending on the edema subtype. Cytotoxic edema was associated with a 92% increased likelihood of poor functional outcomes at six months (adjusted odds ratio 1.92, p=0.002) and, more alarmingly, a greater than threefold increase in the risk of in-hospital death (adjusted odds ratio 3.17, p=0.021)[1]. Global cerebral edema carried an 83% increased likelihood of poor six-month functional outcomes (adjusted odds ratio 1.83, p=0.006). These associations held true even after adjusting for other variables, meaning that the edema subtype itself, not just the overall severity of the stroke, was an independent predictor of the outcome.
The Mechanism: Why Edema Type Matters
To understand why these findings are biologically coherent, it helps to revisit what happens inside the skull when venous drainage fails. When a clot obstructs a major cerebral vein or sinus, venous pressure rises. Blood that should be leaving the brain pools. Initially, this high pressure forces plasma—the liquid component of blood—out through the walls of small blood vessels and into the surrounding brain tissue. This is vasogenic edema: the brain’s architecture is waterlogged, but the neurons themselves are still viable. On magnetic resonance (MR) imaging, this pattern appears as increased signal on certain sequences without a corresponding change on diffusion-weighted imaging[3].
Cytotoxic edema, however, signals a much darker picture. As venous congestion persists or worsens, the tissue’s oxygen supply drops below a critical threshold. Starved of energy, neurons and glial cells can no longer operate the sodium-potassium pumps that maintain their internal environment[4]. Water rushes into the cells, causing them to swell and ultimately rupture. This is irreversible damage; the tissue is dying or dead. On diffusion-weighted MRI, cytotoxic edema produces the characteristic “restricted diffusion” pattern that radiologists recognize as an acute infarct[3]. The threefold mortality increase associated with this subtype is, in retrospect, not surprising: it signals that the brain has transitioned from a state of reversible congestion to one of permanent injury.
Global cerebral edema adds another dimension of danger. When the edema is no longer confined to the territory drained by a single thrombosed vein but involves the brain diffusely, it suggests either widespread venous failure or a secondary process—perhaps a vicious cycle where increased intracranial pressure triggers further venous compression and worsening congestion[5]. This can lead to herniation, where the swollen brain tissue is physically displaced through rigid openings in the skull, compressing the brainstem and threatening life.
Clinical Implications: What These Findings Mean for Practice
The practical takeaway from these findings is as simple as it is important: a radiology report for a patient presenting with CVT should not simply state “cerebral edema present.” The subtype of edema matters. Identifying cytotoxic edema or global swelling on initial imaging can, and probably should, trigger a higher level of monitoring, earlier consideration of endovascular thrombectomy, or more aggressive management of intracranial pressure beyond standard anticoagulation with heparin[6].
A healthy dose of skepticism is also warranted, however. This was a registry-based observational study, not a randomized trial. Registry data, no matter how large, carries inherent limitations: unmeasured confounding factors, variability in imaging protocols between centers, and the impossibility of proving causation. While a sample size of 394 patients is respectable for a rare condition, it limits the precision of subgroup analyses. And most importantly, this study tells us who is at higher risk, but it does not yet tell us whether acting on this information with specific interventions actually changes outcomes. Answering that question will require prospective studies.
Still, for a notoriously unpredictable condition like CVT—where a 25-year-old can present with a headache and walk out of the hospital a week later, or present the same way and die within days—any tool that sharpens early prognosis has real value. The edema subtype, visible on the very first scan, may be one of the most accessible and actionable tools we have.
Scientific Sources
- Brito A, et al. Early Cerebral Edema Subtypes and Functional Outcome in Patients With Cerebral Venous Thrombosis: Insights From the CLOT-VENUS Registry. Neurology. 2026;107(2):e218259. PubMed: https://pubmed.ncbi.nlm.nih.gov/42348805/
- Ulivi L, et al. Cerebral venous thrombosis: a practical guide. Pract Neurol. 2020.
- Schaefer PW, et al. Diffusion-weighted MR imaging of the brain. Radiology. 2000.
- Bhardwaj A, et al. Mechanisms of ischemic brain damage. Curr Cardiol Rep. 2003.
- Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med. 2005.
- Saposnik G, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011.
Medically reviewed by
Dr. Şekip Altunkan
Dr. Şekip Altunkan is an internal medicine specialist with extensive clinical experience. He trained at Hacettepe University Faculty of Medicine and later served as an Associate Professor in Internal Medicine. He founded and led the Metropol Internal Medicine and Hypertension Clinic in Ankara, pioneering non-invasive Electron Beam Tomography (EBT) cardiac imaging, arterial-stiffness measurement, and nationwide Holter monitoring. He currently practices at his private clinic in Ankara, focusing on hypertension, vascular health, cholesterol, diabetes and heart disease. He has published widely in national and international journals, serves as a peer reviewer for several international journals, and is the author of the book "Questions and Answers on Hypertension."