One Disease Wearing Many Masks
Key Takeaway: A groundbreaking series of articles in The Lancet argues that cardiometabolic conditions such as diabetes, heart disease, chronic kidney disease, and stroke share common root causes. Therefore, instead of being treated as isolated illnesses, they should be prevented and managed through a unified, multi-level strategy. Combining population-wide public health measures, individual lifestyle and pharmacological interventions, and integrated healthcare delivery models represents the most promising approach to reducing the global burden of these interconnected disorders.
The Dangerous Cocktail in Plain Sight
In the United States, most individuals over the age of 65 are battling at least two chronic illnesses, a picture that often resembles a dangerous cocktail of heart, kidney, and metabolic disorders. Consider Margaret, a 68-year-old retired teacher. She sees a cardiologist for heart failure, an endocrinologist for type 2 diabetes, and a nephrologist for her declining kidney function. Her primary care physician attempts to reconcile the conflicting medication lists from these three specialists. Margaret takes eleven pills a day, visits four separate clinics, and has received contradictory dietary advice on multiple occasions. Her story is not the exception; it is the norm. And it represents one of the most significant failures of modern medicine: treating each chronic disease as if it exists in a vacuum, even when biology tells us they are deeply and dangerously intertwined.
The Lancet Series: A Closer Look
A comprehensive series of articles published in The Lancet aimed to directly challenge this fragmented approach to medicine by synthesizing the evidence on cardiometabolic multiple long-term conditions (MLTC). This concept describes the clinical clustering of disorders such as type 2 diabetes, coronary artery disease, heart failure, stroke, and chronic kidney disease. Rather than a single clinical trial, this work was an extensive, authoritative review based on decades of epidemiological data, intervention studies, and health systems research, all aimed at proposing a holistic framework for prevention and management[1]. The series identified the need for action on three interconnected levels: societal, individual, and health system. At the societal level, fiscal policies (like sugar taxes), regulatory measures (like limiting trans fats in food production), and environmental changes (like building walkable communities) can shift the risk profile of entire populations. At the individual level, lifestyle interventions—such as structured exercise programs, nutritional counseling, and smoking cessation—combined with pharmacotherapies like statins, SGLT2 inhibitors, and GLP-1 receptor agonists have been proven to reduce both the incidence and progression of cardiometabolic MLTC. At the system level, the series called for integrated care models that treat the patient as a whole, rather than directing them through a maze of disconnected specialists.
Why These Diseases Cluster Together
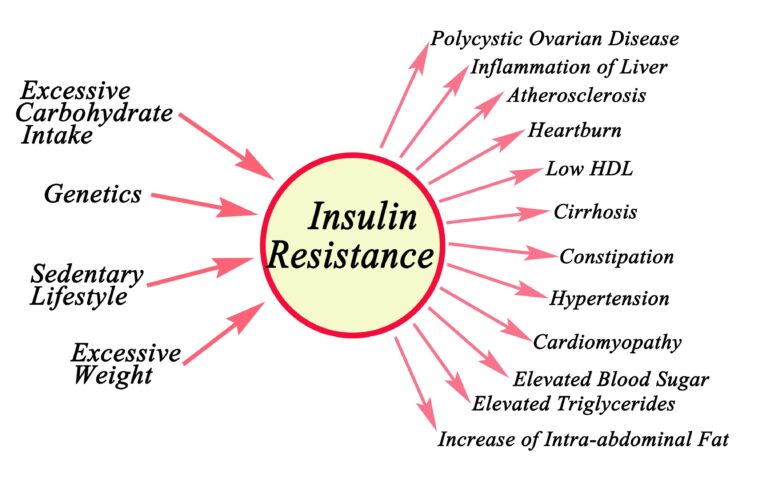
The clustering of cardiometabolic diseases is no coincidence. It is the result of a shared pathophysiology. At the center of this complex web lies insulin resistance, a condition in which cells become less responsive to the signal to take up glucose from the bloodstream. Insulin resistance not only leads to hyperglycemia but also triggers dyslipidemia, endothelial dysfunction, and a chronic, low-grade inflammatory state that accelerates atherosclerosis[2]. The same metabolic soil that allows type 2 diabetes to flourish simultaneously nourishes coronary artery disease and chronic kidney disease.
Chronic inflammation is a key amplifier in this process. Visceral adipose tissue, which surrounds the internal organs, is not a passive storage depot. On the contrary, it is an active endocrine organ that secretes pro-inflammatory cytokines like interleukin-6 and tumor necrosis factor-alpha, molecules that damage blood vessel walls and promote clot formation[3]. Meanwhile, persistently high blood sugar (hyperglycemia) glycates proteins throughout the body, stiffening artery walls and damaging the delicate filtration units in the kidneys known as glomeruli[4]. The hypertension that frequently accompanies these conditions further increases the mechanical stress on this already compromised vasculature.
This shared biology explains why treating one condition in isolation so often fails. If you aggressively lower a patient’s blood sugar but neglect their blood pressure, you might slow their diabetic retinopathy but do nothing to prevent the heart attack that is more likely to kill them. The Lancet series makes a compelling case that only by targeting common upstream drivers—metabolic dysfunction, inflammation, and vascular damage—can we meaningfully alter the course of cardiometabolic multimorbidity.
A Historical Blind Spot
Medicine was not always this compartmentalized. The concept of “metabolic syndrome”—the clustering of central obesity, hypertension, hyperglycemia, and dyslipidemia—was first formally described in 1988 by Gerald Reaven, who posited insulin resistance as the unifying element[5]. Yet despite this recognition over three decades ago, healthcare delivery has remained largely organized around single-disease guidelines, specialists, and research funding. This Lancet series is a call to finally align clinical practice with the reality that biology has been telling us all along.
What This Means for Tomorrow’s Patients
For a patient like Margaret, the practical implications of this framework are profound. An integrated care model would mean a single, coordinated team—perhaps led by a primary care physician specializing in cardiometabolic health—managing her diabetes, heart failure, and kidney disease under one roof, with one medication reconciliation process and one consistent nutrition plan. New classes of drugs are already facilitating this. SGLT2 inhibitors, originally developed for diabetes, have shown remarkable benefits in heart failure and chronic kidney disease, offering the potential to treat three different conditions with a single pill[6]. GLP-1 receptor agonists have demonstrated cardiovascular and renal protective effects that extend far beyond glucose control[7]. These medications are not only practical but also biologically rational, as they target the common metabolic pathways that drive the disease cluster.
At the societal level, the series suggests that upstream interventions could prevent millions from developing multimorbidity in the first place. Countries like Mexico that have implemented taxes on sugar-sweetened beverages have seen measurable reductions in consumption, a change that could translate into lower rates of obesity and diabetes over decades[8].
Limitations to Consider
However comprehensive, no synthesis rewrites clinical practice overnight. The Lancet series is based on existing evidence rather than generating new clinical trial data, and many of the integrated care models it advocates are still in the early stages of implementation. While the evidence for societal-level fiscal policies is promising, it is often derived from short follow-up periods, and the long-term health outcomes of measures like sugar taxes are still being studied. Health systems vary widely between countries, and a model that works in a well-funded national health service may not be easily transferable to fragmented, insurance-driven models. Finally, the series focuses on cardiometabolic conditions and does not fully address the added complexity of co-occurring mental health disorders, cancers, or musculoskeletal diseases that many patients with multimorbidity also face.
The Final Assessment
I have been treating my patients with this kind of holistic approach for 35 years, and I have seen its profound benefits in their lives.
The core message of this Lancet series is both simple and radical: cardiometabolic diseases are a single problem wearing many different masks, and our health systems must stop pretending otherwise. For patients navigating the exhausting labyrinth of multiple specialists, conflicting advice, and polypharmacy, the promise of integrated care built on a foundation of shared biology is not just more efficient—it is more humane. The tools are already available, from societal-level policy levers to medications that simultaneously protect the heart, kidneys, and metabolic health. The harder task that remains is to re-engineer how healthcare is delivered, funded, and coordinated so that the next Margaret can walk into a single clinic, be seen by a single team, and leave with a single plan that truly addresses the interconnected storm raging inside her body.
Scientific Sources
- Valabhji J, et al. Interventions for the prevention and management of cardiometabolic multiple long-term conditions. Lancet (London, England). 2026;407(10548):2668-2684. PubMed: https://pubmed.ncbi.nlm.nih.gov/42259342/
- Reaven GM. Role of insulin resistance in human disease. Diabetes. 1988.
- Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006.
- Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes. 2005.
- Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988.
- McMurray JJV, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019.
- Marso SP, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016.
- Colchero MA, et al. Beverage purchases from stores in Mexico under the excise tax on sugar sweetened beverages. BMJ. 2016.
Medically reviewed by
Dr. Şekip Altunkan
Dr. Şekip Altunkan is an internal medicine specialist with extensive clinical experience. He trained at Hacettepe University Faculty of Medicine and later served as an Associate Professor in Internal Medicine. He founded and led the Metropol Internal Medicine and Hypertension Clinic in Ankara, pioneering non-invasive Electron Beam Tomography (EBT) cardiac imaging, arterial-stiffness measurement, and nationwide Holter monitoring. He currently practices at his private clinic in Ankara, focusing on hypertension, vascular health, cholesterol, diabetes and heart disease. He has published widely in national and international journals, serves as a peer reviewer for several international journals, and is the author of the book "Questions and Answers on Hypertension."