The Silent Siege of Circulation: ApoB in the Atherogenic Lipid Paradigm and Next-Generation Cardiovascular Protection
Key Takeaway: The process of atherosclerosis, which defines the vascular limits of human lifespan, rests upon a complex particle dynamic that cannot be measured solely by the total mass of cholesterol in the plasma, as conventional medicine long assumed. Modern cardiovascular protection is not merely a matter of bulk lipid clearance, but rather the art of managing the absolute number of hazardous particles capable of infiltrating the arterial wall. Especially in clinical scenarios shadowed by insulin resistance and metabolic syndrome, standard lipid panels yield deceptively reassuring results, whereas Apolipoprotein B (ApoB) acts as a singular molecular identity card that exposes the true magnitude of this hidden, residual risk. Today, a therapeutic arsenal spanning from conventional statin regimens to next-generation RNA technologies operating at the cellular level aims to radically dilute this invading army of particles within the vascular wall. Consequently, the future of medicine is evolving beyond simply lowering lipid concentrations toward a sophisticated form of particle management that shields the vascular beds at a molecular level.
Introduction: From Framingham to the Molecular Era—The Ontology of Cholesterol
Ever since humanity discovered that insidious sediment obstructing the beds of its internal rivers, the origins of arterial hardening have been read as a simple story of excess. In the mid-twentieth century, when the initial data from the Framingham Heart Study were laid out on the tables of the medical world, a linear link between total cholesterol elevation and myocardial infarction became the founding dogma of cardiovascular epidemiology. The scientific community viewed this structure, which accumulated within the inner wall of the vessel and calcified over time to narrow the lumen, as a direct consequence of dietary fat intake. In the subsequent decades, the separation of lipoproteins by their densities provided medicine with a more refined definition of friend and foe. Labelled as “bad cholesterol,” LDL cholesterol became the primary target of internal medicine and the absolute ruler of clinical guidelines.
Yet, clinical practice did not always follow the linear trajectories drawn by theory. In outpatient clinics, emergency corridors, and angiography laboratories, physicians encountered a peculiar paradox: thousands of patients whose LDL cholesterol levels were perfectly normal—or even below the safe thresholds targeted by guidelines—suffered their first heart attack or faced widespread arterial occlusions. Conversely, certain individuals whose lipid panels screamed alarm lived long lives with pristine vascular beds.
This paradox forced medical thought to shift from the concept of “cholesterol concentration”—a mass-based measurement—to the structural and quantitative reality of “particle biology.” The entity infiltrating the inner layer of the vessel, undergoing modification there to trigger the immune system, and forming the core of the occlusive plaque was not the free-floating cholesterol molecule itself. They were protein-coated, microscopic lipid vessels transporting hydrophobic lipids that could not otherwise dissolve in water-based blood plasma. And at the helm of these vessels sat a single protein that gave each its structural integrity: Apolipoprotein B. Medicine underwent a profound philosophical and technical shift, moving from weighing the cholesterol cargo to counting the vessels that carried it.
Paradox and Mismatch: The Blind Spots of Standard Measurements and Residual Risk
In clinical lipidology, “mismatch” or “discordance” refers to a scenario where a patient’s laboratory-measured LDL cholesterol concentration contradicts the total number of circulating harmful particles, namely the ApoB level. This phenomenon is far more than a biochemical nuance; it represents a critical clinical fork in the road that directly dictates a patient’s lifespan and treatment success.
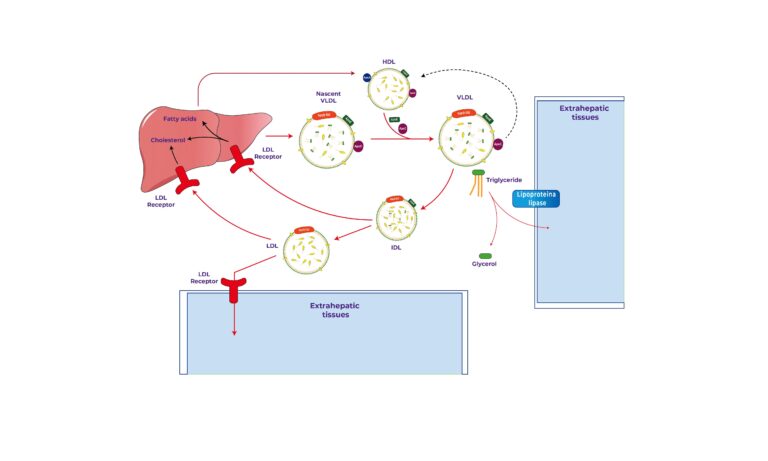
Under normal conditions, when large, cholesterol-rich LDL particles dominate the circulation, the cholesterol value and the ApoB level are concordant; because the amount of cholesterol per particle is high, a elevated cholesterol concentration is measured via a relatively small number of particles. However, when insulin resistance, obesity, type 2 diabetes, or metabolic syndrome enter the equation, the lipid metabolism of the liver and peripheral tissues is fundamentally disrupted. The liver secretes large, triglyceride-rich precursor particles into the bloodstream. These particles interact with other lipids via transfer proteins in the blood plasma, trading away their triglyceride cargo in exchange for cholesterol esters. Subsequently, through the action of specific enzymes, these triglycerides are broken down. The resulting structures are small, dense LDL particles that are reduced in volume, depleted of cholesterol content, but possess a prolonged circulatory lifespan.
In this scenario, because the amount of cholesterol carried within each individual particle is diminished, the total LDL cholesterol concentration measured in routine laboratory testing can appear deceptively low or normal. Yet, every single particle must still carry a single ApoB molecule at its core as a structural requirement. Consequently, a patient whose cholesterol levels appear ideal may harbor more than twice the normal number of small, dense particles in their circulation. This means the patient’s arterial wall is under an onslaught twice as intense, which is the precise, sinsi risk hidden behind a deceptive harmony in laboratory results.
The development of a new vascular event in subsequent years in a patient who has already suffered a heart attack and has been brought to guideline-recommended cholesterol targets under high-dose drug therapy has long occupied the medical community. One of the primary culprits behind this phenomenon, termed residual cardiovascular risk, is an ApoB level that remains elevated despite standard therapy. Classic treatments significantly lower cholesterol mass but may fail to reduce the number of circulating ApoB-bearing particles at the same rate. The arterial wall of a patient deemed a “therapeutic success” by traditional guidelines continues to accumulate lipids beneath the tissue and feed chronic inflammation due to this high particle count.
Therapeutic Strategies and Pharmacodynamic Management
A therapeutic approach targeting ApoB requires not merely emptying the circulating cholesterol pool, but controlling the dynamic lifecycle of all hazardous particles secreted by the liver and destined to end their lifespan in the circulation. This management represents a stepped algorithm that scales from the metabolic reprogramming of lifestyle to the most advanced gene-silencing technologies.
The Molecular Codes of Lifestyle and De Novo Lipogenesis
The primary source of ApoB production is the liver’s capacity to synthesize precursor lipoproteins. This hepatic process is directly tied to the availability of triglycerides and cholesterol within the cell. A major impasse of the modern diet—the excessive consumption of fructose and refined carbohydrates—maximally activates the pathways of de novo lipogenesis (the synthesis of fat from scratch) via specific transcription factors.
When carbohydrate restriction and, in particular, fructose elimination are instituted, the liver’s triglyceride pool rapidly dries up. This suppresses the activity of microsomal triglyceride transfer proteins, which normally stabilize ApoB within the cell after its synthesis, allowing it to achieve a stable configuration. Unable to merge with lipid molecules, the nascent ApoB structures are rapidly degraded by intracellular proteolytic systems before they can be secreted into the blood. Thus, carbohydrate restriction is not a dry dietary recommendation, but a molecular brake that halts the secretion of harmful particles at their source.
The Dynamics of the Classic Arsenal: Sentry and Absorption Synergy
The first line of pharmacotherapy remains the statin class of drugs, which halt cholesterol synthesis. These agents block cholesterol production within the hepatocyte, thereby depleting the intracellular free cholesterol pool. To compensate for this deficit, the cell up-regulates the expression of LDL-capturing receptors on its surface. However, the capacity of these drugs to lower particle numbers when used alone lags behind their capacity to lower cholesterol mass. Under treatment, the liver may continue to secrete a high number of particles that are simply depleted of cholesterol content.
At this juncture, ezetimibe steps in to specifically block the specialized absorption receptors located on the brush border of intestinal cells. Inhibiting the absorption of dietary and biliary cholesterol dramatically reduces the mass of cholesterol returning to the liver. The liver, responding to this cellular cholesterol starvation, further increases the density of capturing receptors on its surface. This combination, besieging both synthesis and absorption simultaneously, synergistically accelerates the clearance rate of circulating ApoB particles.
Next-Generation Targeted Therapies: Technologies Extending Receptor Lifespan
One of the greatest revolutions in lipidology in recent years is the discovery and suppression of an enzyme called PCSK9, which dictates the fate of capturing receptors. In normal physiology, this enzyme binds to LDL receptors on the hepatic surface, triggering their internalization and subsequent degradation in cellular disposal units called lysosomes. This process reduces the number of surface receptors, making the clearance of harmful particles difficult.
If this process is halted through enzyme blockade, the receptors are recycled to the cell surface repeatedly. Hepatic cells achieving maximum receptor density begin to aggressively clear all ApoB-containing particles from the plasma.
- Monoclonal Antibodies (Evolocumab, Alirocumab): Administered subcutaneously at specific intervals, these modern molecules capture free circulating enzymes like a sponge, preventing them from binding to receptors. Consequently, the receptors escape cellular destruction, remain on the surface, and deliver a net reduction in ApoB levels of up to fifty percent.
- Small Interfering RNA (siRNA – Inclisiran): Eliminating compliance issues in treatment, this advanced technology utilizes a synthetic RNA molecule directed straight into the liver cell. With an injection administered just twice a year, the intracellular production of the target enzyme is silenced at the genetic level. The result is a sustained, non-fluctuating, and stable decline in particle numbers.
The Horizon of the Future: Enzymatic Freedom and Direct Synthesis Inhibition
In cases of severe familial hypercholesterolemia or patients exhibiting resistance to conventional therapies, medical science pushes the absolute boundaries of vascular biology.
There exists a specific protein termed Angiopoietin-like 3 (ANGPTL3), which acts as a natural brake on the activity of fat-clearing enzymes in the body. A next-generation treatment, evinacumab, deactivates this inhibitory protein, fully unleashing the activity of these fat-clearing enzymes. This mechanism enables the rapid catabolism of ApoB-containing lipoproteins within the vascular bed, completely independent of traditional capturing receptor function. Even in the most resistant patients harboring receptor mutations, this pathway offers a groundbreaking alternative. Furthermore, antisense oligonucleotide technologies, which directly target and enzymatically destroy the messenger RNAs carrying the production blueprint for ApoB, have demonstrated how potent a therapeutic weapon it can be to dry up particle production at the ribosomal stage—directly at its source.
Molecular Footnotes and Flawless Evidences
The true dramaturgy of atherosclerosis is staged at the scale of one-millionth of a millimeter, within the dim and sheltered space beneath the arterial wall. Every single Apolipoprotein B-100 molecule circulating in the plasma is a massive protein belt comprised of thousands of amino acids, wrapping around the outer shell of the transport vessel like a coat of armor. Upon this protein lie positively charged, specialized amino acid regions that enable it to bind electrostatically to negatively charged sugar structures (proteoglycans) found within the cellular extracellular matrix of the arterial wall once it crosses the innermost endothelial layer. When a hazardous particle from the bloodstream slips through the microscopic junctions between endothelial cells and enters the subendothelial space, it adheres to the matrix like a magnet through the attraction of these positive and negative charges. This adherence is an insidious process of retention that prevents the particle from returning to the active circulation.
Trapped beneath the tissue, these structures fall prey to attacks by aggressive oxygen radicals and enzymes secreted by surrounding cells, transforming into oxidized molecules. Because the three-dimensional conformation of this modified structure is warped, it can no longer be recognized by the normal clearing receptors of the liver. Immune cells (macrophages) migrating into the tissue for defense begin to ingest these alienated structures uncontrollably via their scavenger receptors. Unlike normal receptors, these scavenger systems lack a feedback inhibition or “satiation” mechanism; the process of engulfment persists until the cell is gorged to capacity with intracellular lipid droplets. Ultimately, these immune cells, completely packed with fat, transform into programmed cellular debris that forms the core of the plaque, broadcasts inflammatory signals to the surroundings, and perpetuates vascular destruction—known clinically as foam cells. Consequently, the circulating ApoB concentration is the primary and most faithful determinant of the molecular kinetics that initiate this chain of retention and cellular debris accumulation.
In conclusion, ApoB appears to be a highly informative molecule, particularly in states of diabetes, insulin resistance, obesity, metabolic syndrome, elevated triglycerides, and very low LDL-C concentrations. ApoB accurately reflects the absolute number of atherogenic lipoproteins in circulation and is accepted in many scenarios as a more robust predictor of cardiovascular risk than LDL-C. Current debates reside less in the underlying biology and more in clinical implementation—specifically regarding optimal treatment thresholds and how best to integrate ApoB with other markers like Lp(a). ApoB plays a central mechanistic role in the pathogenesis of atherosclerosis and serves as a clinically powerful biomarker of total atherogenic particle burden. Especially in low LDL-C settings, where cholesterol mass and particle number diverge, it is widely recognized that ApoB provides a superior, individualized reflection of atherosclerotic risk compared to traditional LDL-C metrics.
Our slogan: “The serene light of science renders visible even the most insidious siege within the silent darkness of the vessels; for medicine is not merely a scale that weighs masses, but a wisdom that counts molecular destiny.” — The Vault
Key Clinical Studies & Guidelines Reviewed
- Sniderman AD, et al. Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review of Why ApoB is the Superior Marker. JAMA Cardiology. 2019. PMID:31642874.
- Mach F, et al. (ESC/EAS Guidelines). 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. European Heart Journal, 2020. PMID: 31504418.
- Sabatine, M. S., et al. (FOURIER Investigators). Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. New England Journal of Medicine, 2017. PMID: 28304224.
- Ray KK, et al. (ORION-10 and ORION-11 Trials). Two Phase 3 Trials of Inclisiran in Patients with Cardiovascular Disease. New England Journal of Medicine, 2020. PMID: 32187462.
- Boren J, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel. European Heart Journal, 2020. PMID: 32052833.
- Soffer DE, et al. Role of apolipoprotein B in the clinical management of cardiovascular risk in adults: An Expert Clinical Consensus from the National Lipid Association. Journal of Clinical Lipidology. 2024. PMID: 39256087.
- De Oliveira-Gomes D, et al. Apolipoprotein B: Bridging the Gap Between Evidence and Clinical Practice. Circulation. 2024. PMID: 38950110.
Medically reviewed by
Dr. Şekip Altunkan
Dr. Şekip Altunkan is an internal medicine specialist with extensive clinical experience. He trained at Hacettepe University Faculty of Medicine and later served as an Associate Professor in Internal Medicine. He founded and led the Metropol Internal Medicine and Hypertension Clinic in Ankara, pioneering non-invasive Electron Beam Tomography (EBT) cardiac imaging, arterial-stiffness measurement, and nationwide Holter monitoring. He currently practices at his private clinic in Ankara, focusing on hypertension, vascular health, cholesterol, diabetes and heart disease. He has published widely in national and international journals, serves as a peer reviewer for several international journals, and is the author of the book "Questions and Answers on Hypertension."