The Endothelial Frontier: Why Your Biological Age is the Age of Your Arteries
Key Takeaway: Modern vascular medicine reveals that biological aging is fundamentally dictated by the health of the endothelium, a massive and dynamic endocrine organ whose dysfunction serves as the ground zero for arterial stiffness and atherosclerosis. The onset of vascular destruction hinges on two interconnected molecular phenomena: the loss of endothelial nitric oxide (NO) bioavailability—which deprives vascular smooth muscles of their vital relaxation signal—and the structural degradation of the endothelial glycocalyx, an invisible, gel-like protective barrier. When cardiovascular risk factors like hypertension, diabetes, and oxidative stress disrupt this delicate frontier, they trigger the uncoupling of the eNOS enzyme, turning it from a protective NO factory into a source of toxic free radicals that accelerate chronic vascular remodeling and intima-media thickening. Quantified clinically via non-invasive measures like Pulse Wave Velocity (PWV) and Augmentation Index (AIx), this mechanical stiffening forces pressure waves to reflect prematurely back to the heart, demanding a holistic, multi-pronged therapeutic strategy that combines physical movement, rigorous metabolic control, and pleiotropic agents like statins and ACE inhibitors to restore endothelial flexibility and successfully lower cardiovascular risk.
Introduction: The Largest and Most Active Organ in the Body
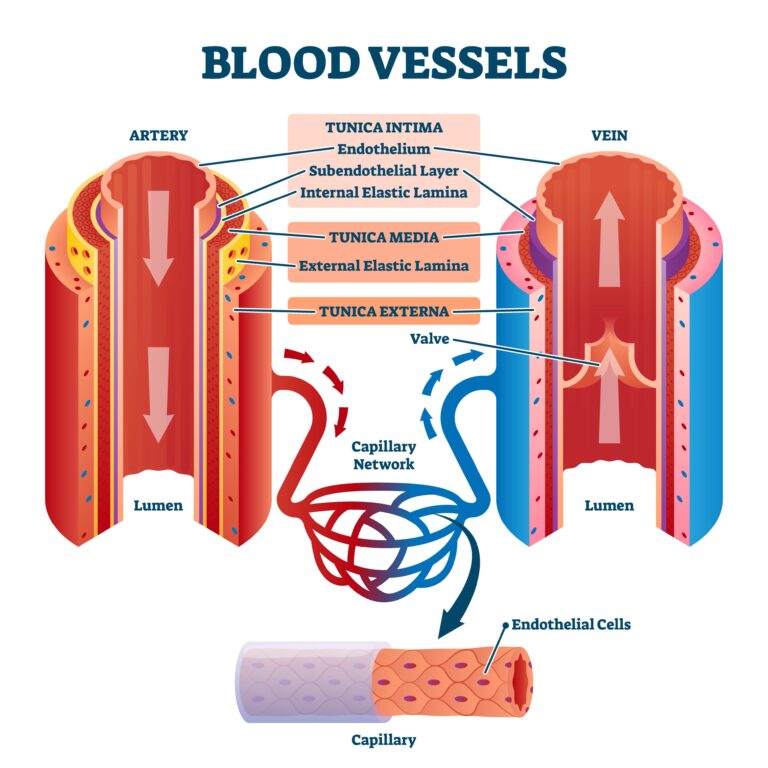
For a long time, medical textbooks viewed the layer of cells lining the interior of the vessels—the Endothelium—as merely a passive “Teflon coating” that facilitated blood flow. Today, however, we know that the endothelium is a dynamic and massive endocrine organ, distributed throughout the body, with a total weight comparable to that of the liver. No matter how strong your heart may be, if your endothelium is not performing its duty, it is impossible for blood to reach the tissues.
Endothelial dysfunction plays a pivotal and early role in vascular aging, arterial stiffness, and atherosclerotic disease. The most critical findings in recent research highlight the loss of bioavailability of Nitric Oxide (NO) produced by the endothelium and the degradation of the Endothelial Glycocalyx. These two events interact in a vicious cycle that promotes arterial stiffness, inflammation, and cardiovascular events, ultimately leading to vascular damage.
In this chapter of “The Vault,” we will focus on “Ground Zero” of vascular health: endothelial function and the mechanics of arterial stiffness.
Nitric Oxide (NO): The “Respiration” of the Vessels
The most vital task of endothelial cells is the production of the Nitric Oxide (NO) molecule, a discovery that earned the Nobel Prize in 1998. NO is the primary signal that commands vascular smooth muscles to “relax.”
- Vasodilation Capacity: A healthy endothelium immediately secretes NO when blood flow increases (e.g., during exercise) to dilate the vessel. The loss of this capacity is termed “Endothelial Dysfunction” and is the starting point of all vascular destruction.
- Anti-Atherogenic Protection: NO does more than just dilate vessels; it acts as a “security shield” that prevents platelets from adhering to the vascular wall (clot formation) and stops cholesterol from leaking into the vessel.
The Glycocalyx: The Invisible Armor of the Endothelium
On the surface of endothelial cells that comes into contact with the blood, there lies a gel-like layer that the medical world is only beginning to fully understand: The Endothelial Glycocalyx.
- Vascular Sieve: This hair-like structure protects the vascular wall from the onslaught of leukocytes (inflammatory cells).
- Signal Transducer: This structure is also critically important for stimulating the release of NO.
- Leakage and Edema: Risk factors that cause arterial stiffness effectively “mow down” this delicate forest. When the glycocalyx is damaged, the vessel begins to leak, leading to tissue edema and triggering arterial stiffness. Glycocalyx health is the most critical element determining the “hydraulic resistance” of the vessel.
- The Vicious Cycle: Animal studies demonstrate that even before plaques form, glycocalyx loss, increased endothelial stiffness, decreased NO production, and increased permeability occur simultaneously. This suggests a mutually reinforcing cycle that initiates damage rather than a simple linear sequence.
Arterial Stiffness and Pulse Wave Velocity (PWV)
Vascular flexibility is the most significant physical parameter determining the load on the heart. The heart creates a pressure wave with every contraction; if the vessels are stiff, this wave travels very rapidly and “reflects back” to the heart prematurely, fatiguing the organ.
- Pulse Wave Velocity (PWV): This is an indirect test used to measure arterial stiffness. The faster a pressure wave travels within the vessel, the stiffer your arteries have become.
- Augmentation Index (AIx): This represents the impact of the reflected pressure wave on the primary wave. A high AIx is a mechanical defect that impairs the heart’s nourishment during the relaxation (diastole) phase, directly increasing the risk of coronary artery disease.
Vascular Remodeling: The Adaptive Response to Pressure
The vascular wall physically alters its structure in response to mechanical stress (pressure and shear stress).
- Intima-Media Thickening (IMT): Under persistent high pressure, the middle layer of the vessel (the media) thickens (remodeling). While initially a protective adaptation, it eventually narrows the vessel lumen and completely eliminates flexibility. We detect this non-invasively through Carotid Doppler Ultrasonography.
- Direct Measurements: Other methods directly measure vascular hardening, such as the Coronary Artery Calcium (CAC) scan, which identifies calcification within the heart’s vessels.
- Reversibility: Many patients ask, “Is there no going back once my vessels have stiffened?” Clinical studies show that through intensive endothelial-protective therapy and lifestyle interventions, these structural changes in the vascular wall can be partially reversed.
“The Endothelium is the Brain of the Vessel”
In the clinic, when examining a patient with arterial stiffness, I don’t just see a clogged pipe; I see a “biochemical factory making the wrong decisions.” If endothelial dysfunction has set in, the vessel can no longer manage the blood; it merely resists it.
I always use this analogy with my patients: “Your vessels should be as flexible as a garden hose; if that hose is left in the sun and turns into a stiff plastic pipe, it will eventually crack, regardless of the water pressure passing through it.” Therefore, our primary goal in treatment is not just to lower cholesterol, but to restore the endothelium’s miraculous NO production. As a physician, I must prescribe more than just medication; I must include “movement”—the endothelium’s favorite drug. Attention to diet and the management of comorbid chronic diseases are equally vital. Here, I must emphasize the importance of anti-cholesterol therapy; cholesterol-lowering drugs have numerous beneficial effects on arterial stiffness and endothelial dysfunction. The treatment of hypertension and diabetes is also paramount in this regard.
Remember: Fluid blood and flexible vessels are the unchanging equation for a healthy life.
The Target: “Coupling” the eNOS Enzyme and Redox Balance
At the heart of endothelial health lies the eNOS (endothelial nitric oxide synthase) enzyme. Under normal conditions, this enzyme produces NO; however, under oxidative stress and inflammation, it becomes “uncoupled” (eNOS uncoupling). In this state, instead of producing protective NO, the enzyme begins to produce free radicals that “burn” the vascular wall. So, what is done in treatment?
- Classic Therapies: ACE inhibitors and statins do more than just lower blood pressure and cholesterol; they exhibit pleiotropic protective effects on the endothelium, supporting eNOS function.
- Enzymatic Repair: The focus of modern medicine is to repair the eNOS enzyme directly rather than simply replacing NO from the outside. Specific activators and stimulators that target damaged or inactive forms of eNOS offer the potential to restore vascular health safely, without the risk of “overdosing.”
- Redox Switches and BH_4: For eNOS to function correctly, the management of “redox switches” and cofactors like BH_4 (Sapropterin) is essential. Site-specific antioxidant therapies in this field aim to preserve the delicate molecular balance within the vascular wall.
Conclusion: To Preserve Flexibility is to Preserve Life
Vascular health is not a status, but a balance that must be continuously protected. Protecting the endothelial frontier requires managing blood pressure, controlling inflammation, and understanding vascular mechanics. Remember, no matter how strong your heart may be, you are only as free as the flexibility of your vessels.
Let’s define our slogan with this vascular truth: “Vascular flexibility is the flexibility of life; take good care of your endothelium—it is your greatest ally.”
Key Clinical Studies & Guidelines Reviewed
- Bonetti PO, Lerman LO, Lerman A. Endothelial dysfunction: a marker of atherosclerotic risk. Arterioscler Thromb Vasc Biol. 2003 Feb 1;23(2):168-75.
- Vlachopoulos C, et al. Prediction of Cardiovascular Events and All-Cause Mortality With Arterial Stiffness: A Systematic Review and Meta-Analysis. J Am Coll Cardiol. 2010 Mar 30;55(13):1318-27.
- Nieuwdorp M, et al. Endothelial glycocalyx damage coincides with microalbuminuria in type 1 diabetes. Diabetes. 2006;55(4):1127-1132.
- Libby P, Ridker PM, Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature. 2011;473(7347):317-325.
- Daiber A, et al. New Therapeutic Implications of Endothelial Nitric Oxide Synthase (eNOS) Function/Dysfunction in Cardiovascular Disease. Int J Mol Sci. 2019 Jan 7;20(1):187.
Medically reviewed by
Dr. Şekip Altunkan
Dr. Şekip Altunkan is an internal medicine specialist with extensive clinical experience. He trained at Hacettepe University Faculty of Medicine and later served as an Associate Professor in Internal Medicine. He founded and led the Metropol Internal Medicine and Hypertension Clinic in Ankara, pioneering non-invasive Electron Beam Tomography (EBT) cardiac imaging, arterial-stiffness measurement, and nationwide Holter monitoring. He currently practices at his private clinic in Ankara, focusing on hypertension, vascular health, cholesterol, diabetes and heart disease. He has published widely in national and international journals, serves as a peer reviewer for several international journals, and is the author of the book "Questions and Answers on Hypertension."